|
Overview
Adult acquired flat foot was first described in the late 1960s as something that occurred after trauma, as a result of a tear to the tibial posterior tendon. However, by 1969 two doctors called Kettlekamp and Alexander described cases in which no trauma had taken place. They referred to the condition as "tibial posterior tendon dysfunction" and this became known as the most common type of adult acquired flat foot.  Causes A person with flat feet has greater load placed on the posterior tibial tendon which is the main tendon unit supporting up the arch of the foot. Throughout life, aging leads to decreased strength of muscles, tendons and ligaments. The blood supply diminishes to tendons with aging as arteries narrow. Heavier, obese patients have more weight on the arch and have greater narrowing of arteries due to atherosclerosis. In some people, the posterior tibial tendon finally gives out or tears. This is not a sudden event in most cases. Rather, it is a slow, gradual stretching followed by inflammation and degeneration of the tendon. Once the posterior tibial tendon stretches, the ligaments of the arch stretch and tear. The bones of the arch then move out of position with body weight pressing down from above. The foot rotates inward at the ankle in a movement called pronation. The arch appears collapsed, and the heel bone is tilted to the inside. The deformity can progress until the foot literally dislocates outward from under the ankle joint. Symptoms Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot. Diagnosis Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered. Non surgical Treatment Depending on the stage of the deformity and patient?s functional goals, various treatment options are available. Some patients improve with conservative care which includes rest and immobilization, shoe modifications, orthoses and bracing, or physical therapy. Surgery might be warranted for advanced stages of the condition. Often a combination of procedures including tendon and muscle augmentation, tendon transfers, realigning of bones or fusion of certain joints might be necessary in more advanced cases. Your doctor will evaluate and recommend an individualized plan of care with your specific needs in mind.  Surgical Treatment Types of surgery your orthopaedist may discuss with you include arthrodesis, or welding (fusing) one or more of the bones in the foot/ankle together. Osteotomy, or cutting and reshaping a bone to correct alignment. Excision, or removing a bone or bone spur. Synovectomy, or cleaning the sheath covering a tendon. Tendon transfer, or using a piece of one tendon to lengthen or replace another. Having flat feet is a serious matter. If you are experiencing foot pain and think it may be related to flat feet, talk to your orthopaedist. Overview
A fallen arch or flatfoot is known medically as pes planus. The foot loses the gently curving arch on the inner side of the sole, just in front of the heel. If this arch is flattened only when standing and returns when the foot is lifted off the ground, the condition is called flexible pes planus or flexible flatfoot. If the arch disappears in both foot positions, standing and elevated, the condition is called rigid pes planus or rigid flatfoot.  Causes Plantar fasciitis, another sports injury detailed on this website, is regularly the cause of foot arch pain or strain. This can arise due to faulty biomechanics in your feet, which alone can also provoke foot arch pains. The most prominent biomechanical difficulties are flat feet and high arches. With flat feet (or overpronation) the arches appear to be almost flattened, causing unevenness by forcing the feet roll inwards in order to maintain balance and support the body's weight. This places inordinate pressure on the plantar fascia and arches. If by contrast you have high arches (instep), the ankle can roll outwards, again causing undue strain on the arches. Too much of this strain can lead to stretching of the plantar fascia and pain in the arches. Other causes include overstretching or otherwise pressuring the arches, for example by exercising with fatigued leg muscles which leave the feet with excessive work to do. You are also particularly at risk if in your 40s or 50s and commencing an intense program of training after a long period of inactivity. Symptoms Arch pain symptoms could include any of the following, a dull, constant ache if the ligaments have been stretched, swelling or tenderness in the foot, redness or bruising in the event of a more serious injury, difficulty putting weight on the foot, sharp pain when the foot is turned or manipulated, tenderness when pressure is applied. Because the arch of the foot is such a complex structure, arch pain could be an indicator of several different types of injuries. Chronic illnesses such as arthritis could also cause arch pain, and depending on the cause or source of your pain, you may experience discomfort in a variety of different areas. Ask a doctor if you believe you may have injured your foot arch. Diagnosis The doctor will examine your feet for foot flexibility and range of motion and feel for any tenderness or bony abnormalities. Depending on the results of this physical examination, foot X-rays may be recommended. X-rays are always performed in a young child with rigid flatfeet and in an adult with acquired flatfeet due to trauma. Non Surgical Treatment Flat feet in a child do not need treatment if they are not causing pain or walking problems. Your child's feet will grow and develop the same, whether special shoes, shoe inserts, heel cups, or wedges are used. Your child may walk barefoot, run or jump, or do any other activity without making the flat feet worse. In older children and adults, flexible flat feet that do not cause pain or walking problems do not need further treatment. If you have pain due to flexible flat feet, the following may help. An arch-support (orthotic) that you put in your shoe. You can buy this at the store or have it custom-made. Special shoes. Rigid or painful flat feet need to be checked by a health care provider. The treatment depends on the cause of the flat feet. For tarsal coalition, treatment starts with rest and possibly a cast. Surgery may be needed if pain does not improve. In more severe cases, surgery may be needed to clean or repair the tendon, fuse joints in the foot into a corrected position. Flat feet in older adults can be treated with pain relievers, orthotics, and sometimes surgery. 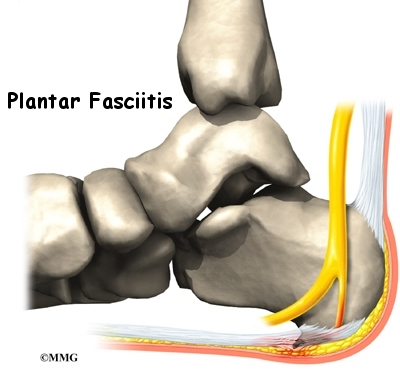 Surgical Treatment Surgery may be necessary in situations where the symptoms are likely to get worse over time, or when pain and instability cannot be corrected with external orthopedic devices. There are many types of surgical procedures, including cavus foot reconstruction, which can be performed to correct the foot and the ankle and restore function and muscle balance. Prevention To prevent arch pain, it is important to build up slowly to your exercise routine while wearing arch supports inside training shoes. By undertaking these simple measures you can prevent the discomfort of arch pain which can otherwise linger for many months. While you allow the foot to recover, it will help to undertake low impact exercises (such as swimming or water aerobics). Stretching Exercises Massage therapy is a great way to loosen muscles and help improve mobility in in your feet. As many people with foot pain have discovered, tight muscles in your legs or back can lead to tense foot muscles. All those muscles are connected, so tension in your back can cause tension in your legs which can pull the tendons in your feet and cause stiffness and pain. Getting acupuncture or a professional full body massage are probably the best ways to deal with this, but there are also some simple tricks you can do at home to help keep muscles limber. These are great for loosening up and improving circulation, both before and after exercise. Place a tennis ball under the arch of your bare foot and roll it around, stretching the muscles in your foot and promoting blood flow. You can also roll the ball under your calves and upper legs to work out stiffness and knots. If you feel the tennis ball is too easy, try a lacrosse ball for deeper massaging. This is also demonstrated in the exercise video above. Use a foam roller, those big overpriced rolls of foam that are now available in every department and sporting goods store are fantastic for self-massage (why a roll of foam costs $30 is beyond us, but they do work wonders-our advice is to not waste money on the more expensive fancy grooved ones because even the simplest rollers work great). The exercises you can do with foam rollers seem to be endless, and there are literally hundreds of free videos online showing how to use them to massage every part of your body. Here's one we picked out that specifically targets foot and leg muscles related to arches and plantar fasciitis.
Overview
 The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1. Causes The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture. Symptoms It is important to know that pain at the back of the heel is not always due to Achilles tendon rupture. It may be due to bursitis (fluid accumulation in the heel due to repeated irritation) and tendonitis (pain along the Achilles tendon due to constant friction and irritation). The above disorders tend to improve with use of pain medications and rest, whereas Achilles tendon rupture requires surgery and/or a cast. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture. The Achilles tendon is the tough sinew that attaches the calf muscle to the back of the calcaneus, or heel bone. It is also known as the tendo calcaneus or the tendo Achilles and happens to be one of the longest tendons in the body. An Achilles tendon rupture occurs when the Achilles tendon is partially or completely broken or torn. The average age of patients who suffer Achilles tendon ruptures is 30 to 40 years. The male-to-female ratio is nearly 20 to 1. Causes The Achilles tendon usually ruptures as a result of a sudden forceful contraction of the calf muscles. Activities such as jumping, lunging, or sprinting can cause undue stress on the Achilles tendon and cause it to rupture. Often there is a background of Achilles tendinitis. Direct trauma to the area, poor flexibility or weakness of the calf muscles or of the Achilles tendon and increasing age are some of the other factors that are associated with an Achilles tendon rupture. Symptoms It is important to know that pain at the back of the heel is not always due to Achilles tendon rupture. It may be due to bursitis (fluid accumulation in the heel due to repeated irritation) and tendonitis (pain along the Achilles tendon due to constant friction and irritation). The above disorders tend to improve with use of pain medications and rest, whereas Achilles tendon rupture requires surgery and/or a cast. Diagnosis In diagnosing an Achilles tendon rupture, the foot and ankle surgeon will ask questions about how and when the injury occurred and whether the patient has previously injured the tendon or experienced similar symptoms. The surgeon will examine the foot and ankle, feeling for a defect in the tendon that suggests a tear. Range of motion and muscle strength will be evaluated and compared to the uninjured foot and ankle. If the Achilles tendon is ruptured, the patient will have less strength in pushing down (as on a gas pedal) and will have difficulty rising on the toes. The diagnosis of an Achilles tendon rupture is typically straightforward and can be made through this type of examination. In some cases, however, the surgeon may order an MRI or other advanced imaging tests. Non Surgical Treatment A medical professional will take MRI scans to confirm the diagnosis and indicate the extent of the injury. Sometimes the leg is put in a cast and allowed to heal without surgery. This is generally not the preferred method, particularly for young active people. Surgery is the most common treatment for an achilles tendon rupture.  Surgical Treatment Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under ?Procedure? in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar. Surgical Treatment Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under ?Procedure? in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
Overview
 The appearance of flat feet is normal and common in infants, partly due to "baby fat" which masks the developing arch and partly because the arch has not yet fully developed. The human arch develops in infancy and early childhood as part of normal muscle, tendon, ligament and bone growth. Training of the feet, especially by foot gymnastics and going barefoot on varying terrain, can facilitate the formation of arches during childhood, with a developed arch occurring for most by the age of four to six years. Flat arches in children usually become proper arches and high arches while the child progresses through adolescence and into adulthood. Causes Fallen arches can be the result of other conditions such as overuse, stretching or tearing of the posterior tibial tendon (which attaches to a bone in the foot and runs up the calf of the lower leg at a tension which pulls up the arch) which reduces its ability to maintain tension in the tendon. Whether or not the condition is caused by overpronation, this is the likely outcome for runners, whose arches are no longer strong enough to take the constant strain of bearing the body?s weight on impact, causing joint, postural and muscular problems. Symptoms A significant number of people with fallen arches (flat feet) experience no pain and have no problems. Some, however, may experience pain in their feet, especially when the connecting ligaments and muscles are strained. The leg joints may also be affected, resulting in pain. If the ankles turn inwards because of flat feet the most likely affected areas will be the feet, ankles and knees. Some people have flat feet because of a developmental fault during childhood, while others may find that the problem develops as they age, or after a pregnancy. There are some simple devices which may prevent the complications of flat feet. Diagnosis There are a few simple ways to assess your foot type, and most include making an imprint of your footprint. The classic way is to stand on a hard floor surface with wet feet to make a wet foot print. Look at the narrowest part of your footprint, which should be between your heel and ball of your foot. If the print of your foot in this part is less than 10% of the width of the widest part then you are likely to have high arches. more than 10% but less than 25% then your foot profile is probably normal, more than 25% or even the widest part, then you have flat feet. Non Surgical Treatment Normally, flat feet disappear by age six as the feet become less flexible and the arches develop. Only about 1 or 2 out of every 10 children will continue to have flat feet into adulthood. For children who do not develop an arch, treatment is not recommended unless the foot is stiff or painful. Shoe inserts won?t help your child develop an arch, and may cause more problems than the flat feet themselves. However, certain forms of flat feet may need to be treated differently. For instance, a child may have tightness of the heel cord (Achilles tendon) that limits the motion of his foot. This tightness can result in a flat foot, but it usually can be treated with special stretching exercises to lengthen the heel cord. Rarely, a child will have truly rigid flat feet, a condition that can cause problems. Surgical Treatment  Surgical procedures for flat feet vary depending on the root cause of the condition. Surgical correction to control pronation may include bone implants or Achilles tendon lengthening. Tendon transfer, which is a procedure to re-attach a tendon to another area of bone, may also be used to reduce pronation and improve foot function. Overview
 Flat Feet and Fallen Arches are terms used to describe feet that have a low or no arch when weight bearing. There are two types of Flat Feet. Rigid Flat Foot. This type of foot is structurally flat, therefore, it has the same appearance when weight bearing and non weight bearing. Flexible Flat Foot. This is where the arch is present when non-weight bearing; however, when weight bearing it falls or collapses to a flat foot. This foot type is commonly referred to as Fallen Arches. Both of these foot types may be asymptomatic; however, they are characterised by excessive pronation of the joints of the foot (commonly the subtalar joint). The forces associated with this excessive pronation commonly results in pathological conditions, such as plantar fasciitis and tibialis posterior dysfunction which may cause pain in the feet. Causes The direct cause of being flat footed is linked to a muscular imbalance in the intrinsic muscles of the foot and ankle. When your main arch-supporting tendon, the posterior tibial tendon, decreases in strength due to muscle decay or injury, the foot begins to flatten and can cause pain during normal activities. Weakness in the tendon can be present at birth due to genetics or can develop from early walking patterns. However, in most people who experience fallen arches, it comes from strain due to aging or placed on the feet from standing or walking in heels for long periods of time. Improper footwear that doesn?t support the arch of the foot, diabetes and obesity can increase your risk of developing fallen arches. Symptoms Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor. Diagnosis Flat feet are easy to identify while standing or walking. When someone with flat feet stands, their inner foot or arch flattens and their foot may roll over to the inner side. This is known as overpronation. To see whether your foot overpronates, stand on tiptoes or push your big toe back as far as possible. If the arch of your foot doesn't appear, your foot is likely to overpronate when you walk or run. It can be difficult to tell whether a child has flat feet because their arches may not fully develop until they're 10 years of age. Non Surgical Treatment The simplest form of treatment is the use of custom fitted orthotics. For this, it is best to see a podiatrist, who is a trained medical professional that assesses feet and gives you a prescription for the orthotic. If the orthotics do not work - or if the deformity is very severe - then surgical management may be needed. There is a very wide range of procedures available, with varying downtimes and complexity. The simplest procedure of all is a simple calf release. This can be done at the back of the knee or the calf, and has a very quick recovery. It is a day-surgery procedure, and the patient can walk immediately after the surgery without the need for a cast. Recovery back to jogging can be as early as three weeks. The calf release stops the deforming force but obviously does not correct the arch itself. It is usually done in combination with some of the other procedures mentioned below. Done by itself, the patient will probably still require orthotics but by releasing the calf, it allows the orthotics to be much more effective. The other end of the spectrum is a complete reconstruction of the arch with bone work and screws to fuse joints. Surgical Treatment  Surgery is typically offered as a last resort in people with significant pain that is resistant to other therapies. The treatment of a rigid flatfoot depends on its cause. Congenital vertical talus. Your doctor may suggest a trial of serial casting. The foot is placed in a cast and the cast is changed frequently to reposition the foot gradually. However, this generally has a low success rate. Most people ultimately need surgery to correct the problem. Tarsal coalition. Treatment depends on your age, extent of bone fusion and severity of symptoms. For milder cases, your doctor may recommend nonsurgical treatment with shoe inserts, wrapping of the foot with supportive straps or temporarily immobilizing the foot in a cast. For more severe cases, surgery is necessary to relieve pain and improve the flexibility of the foot. Lateral subtalar dislocation. The goal is to move the dislocated bone back into place as soon as possible. If there is no open wound, the doctor may push the bone back into proper alignment without making an incision. Anesthesia is usually given before this treatment. Once this is accomplished, a short leg cast must be worn for about four weeks to help stabilize the joint permanently. About 15% to 20% of people with lateral subtalar dislocation must be treated with surgery to reposition the dislocated bone. After Care Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon. Overview
 Achilles tendinitis is an inflammation of your Achilles tendon. It?s quite common in people who have psoriatic arthritis, reactive arthritis or ankylosing spondylitis. It can also occur as an over-use injury in people who take part in excessive exercise or exercise that they?re not used to. Achilles tendinitis is an inflammation of your Achilles tendon. It?s quite common in people who have psoriatic arthritis, reactive arthritis or ankylosing spondylitis. It can also occur as an over-use injury in people who take part in excessive exercise or exercise that they?re not used to.Causes Achilles tendinitis is usually caused by straining the Achilles tendon through intense activity or a sudden increase in exercise. Individuals who play basketball often develop Achilles tendinitis as a result of pivoting, jumping, and running. These repetitive movements put pressure on the tendon and can gradually wear it down over time. Increasing the intensity of your workouts may also lead to the development of Achilles tendinitis. This is commonly seen in long distance runners who do quite a bit of uphill running. Similarly, if you start exercising more frequently you may also develop the condition due to overuse of the tendon. Not stretching properly before exercise can also make the tendon more prone to injury. Achilles tendinitis is also common in individuals whose feet have a flattened arch, as this places more stress on the tendon. The condition can also be triggered by arthritis, as joint pain can cause one to compensate by putting more pressure on the Achilles tendon. Symptoms People with achilles tendinitis experience mild aching on the back of the leg close to the heel after increased activity. Stiffness in the back of the ankle when you first wake up in the morning, which subsides after mild activity. In some cases, the area may have swelling, thickening or be warm to the touch. Tenderness to touch along the tendon in the back of the ankle. Pain when the tendon is stretched (i.e. when you lift your foot/toes up). Diagnosis A podiatrist can usually make the diagnosis by clinical history and physical examination alone. Pain with touching or stretching the tendon is typical. There may also be a visible swelling to the tendon. The patient frequently has difficulty plantarflexing (pushing down the ball of the foot and toes, like one would press on a gas pedal), particularly against resistance. In most cases X-rays don't show much, as they tend to show bone more than soft tissues. But X-rays may show associated degeneration of the heel bone that is common with Achilles Tendon problems. For example, heel spurs, calcification within the tendon, avulsion fractures, periostitis (a bruising of the outer covering of the bone) may all be seen on X-ray. In cases where we are uncertain as to the extent of the damage to the tendon, though, an MRI scan may be necessary, which images the soft tissues better than X-rays. When the tendon is simply inflamed and not severely damaged, the problem may or may not be visible on MRI. It depends upon the severity of the condition. Nonsurgical Treatment As with all conditions, your Doctor should be consulted. Even minor symptoms can represent significant damage to the Achilles tendon. It is recommended that medical advice be sought as soon as symptoms are experienced. Applying ice to the injury on a regular basis can reduce inflammation associated with Achilles Tendonosis. Following the initial injury, ice should be applied for periods of 15 minutes every hour. Resting the injured ankle may be necessary. This can be a problem for athletes who need to train regularly. The degree of rest required depends on the severity and type of Achilles Tendonosis. Your Health Care Professional will advise you about what activities should be limited while the injury is repairing. Fast uphill and downhill running is not advised while an Achilles Tendinosis injury is healing. Anti-inflammatory, analgesic medications such as those containing aspirin may help control pain and inflammation. Self-massage with heat-inducing creams and liniments may be of assistance. Wearing heel-lifts or pads in shoes can reduce the tension in the Achilles tendon. Physiotherapy may assist in the repair of a damaged Achilles tendon. Physiotherapists may recommend exercises to strengthen the tendon to reduce the chances of future injury. Regular stretching of the hamstring muscles (at the back of the calf) can help the repair process. This should only be done when the injury has repaired enough not to cause pain during this stretching. Taping the ankle and wearing appropriate running shoes may help to control movement in the ankle and prevent further injury.  Surgical Treatment There are two types of Achilles repair surgery for tendonitis (inflammation of the Achilles Tendon), if nonsurgical treatments aren't effective. Gastrocnemius recession - The orthopaedic surgeon lengthens the calf muscles to reduce stress on your Achilles tendon. D?bridement and repair - During this procedure, the surgeon removes the damaged part of the Achilles tendon and repairs the remaining tendon with sutures or stitches. Debridement is done when the tendon has less than 50% damage. Prevention So what are some of the things you can do to help prevent Achilles Tendinitis? Warm Up properly: A good warm up is essential in getting the body ready for any activity. A well structured warm up will prepare your heart, lungs, muscles, joints and your mind for strenuous activity. Balancing Exercises, Any activity that challenges your ability to balance, and keep your balance, will help what's called proprioception, your body's ability to know where its limbs are at any given time. Plyometric Training, Plyometric drills include jumping, skipping, bounding, and hopping type activities. These explosive types of exercises help to condition and prepare the muscles, tendons and ligaments in the lower leg and ankle joint. Footwear, Be aware of the importance of good footwear. A good pair of shoes will help to keep your ankles stable, provide adequate cushioning, and support your foot and lower leg during the running or walking motion. Cool Down properly, Just as important as warming up, a proper cool down will not only help speed recovery, but gives your body time to make the transition from exercise to rest. Rest, as most cases of Achilles tendinitis are caused by overuse, rest is probably the single biggest factor in preventing Achilles injury. Avoid over training, get plenty of rest; and prevent Achilles tendinitis. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
July 2017
Categories |
 RSS Feed
RSS Feed
